Metabolic acidosis
Notes
Overview
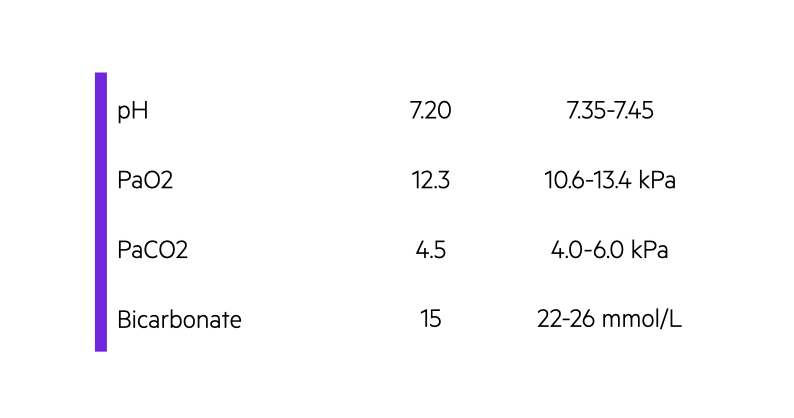
Metabolic acidosis is characterised by a pH < 7.35 and reduced plasma bicarbonate level (< 22 mmol/L).
Metabolic acidosis is one of the most common acid-base abnormalities seen in clinical practice. It is characterised by acidosis (pH < 7.35) and a low plasma bicarbonate level (< 22 mmol/L).
Metabolic acidosis, put simply, can be from a primary increase in hydrogen ions (e.g. addition of strong acid) or reduction in bicarbonate concentration:
- Addition of acid (e.g. diabetic ketoacidosis or methanol ingestion)
- Loss of bicarbonate (e.g. diarrhoea or renal loss)
Determining the cause
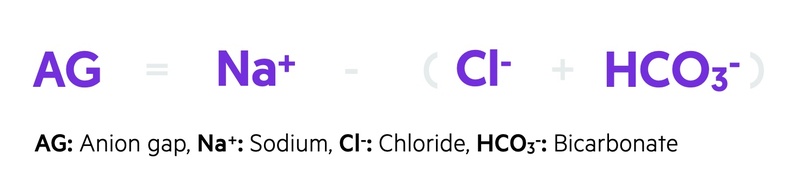
There are numerous causes of metabolic acidosis. These are broadly differentiated based on the anion gap. The anion gap is the difference between the major measured cation sodium (Na+) and anions chloride (Cl-) and bicarbonate (HCO3-).
The aetiology is critical because the fundamental management is identification and treatment of the underlying cause.
Anion gap
The anion gap refers to the difference between the major measured cation sodium and anions chloride and bicarbonate.
The anion gap can be calculated by subtracting the sum of chloride (Cl-) and bicarbonate (HCO3-) from sodium (Na+).
The normal anion gap is approximately 6-12 mEq/L.
The normal anion gap is due to the difference between unmeasured anions (e.g. sulphate, phopshate, albumin, organic anions) and cations (e.g. potassium, magnesium, calcium). Therefore, fluctuations in these unmeasured anions and cations may influence the anion gap.
- Increase in unmeasured anions (e.g. organic acid): leads to ‘consumption’ of bicarbonate and rise in anion gap
- Decrease in unmeasured anions (e.g. hypoalbuminaemia): reduces anion gap
- Increase in unmeasured cations (e.g. hypercalcaemia): reduces anion gap
- Decrease in unmeasured cations (e.g. hypokalaemia): increases anion gap
Anion gap and acidosis
In the context of metabolic acidosis, the anion gap essentially indicates whether there has been an accumulation of unmeasured anions (e.g. organic acids), which subsequently consume bicarbonate due to its buffering ability.
This concept is used to differentiate the causes of metabolic acidosis into ‘normal anion gap acidosis’ and ‘raised anion gap acidosis’.
- Normal anion gap metabolic acidosis (NAGMA): no accumulation of anions. Bicarbonate levels fall due to loss. Compensatory increase in chloride ions. Anion gap maintained.
- High (rasied) anion gap metabolic acidosis (HAGMA): accumulation of anions. Bicarbonate is consumed. Anion gap is raised.
Normal anion gap acidosis
Normal anion gap acidosis is commonly due to renal or GI bicarbonate losses.
Often referred to as normal anion gap metabolic acidosis (NAGMA)
A normal anion gap acidosis describes metabolic acidosis (pH < 7.35) with a normal anion gap (6-12 mEq/L).
In normal anion gap acidosis, there is loss of bicarbonate in the absence of anion generation. There is a reciprocal increase in chloride concentration to maintain electroneutrality (i.e. maintain equal state between positive and negative ions). This increase in chloride is why it is also termed hyperchloraemic metabolic acidosis.
Normal anion gap acidosis is usually due to renal or GI losses of bicarbonate. In practice, it is commonly seen with excess use of normal saline due to the high chloride load. The causes of a normal anion gap acidosis can be remembered using the mnemonic HARDUPS:
- H - hyperalimentation (i.e. delivery of nutrients into a vein): typically due to excess normal saline solution.
- A - acetazolamide: carbonic anhydrase inhibitor
- R - renal tubular acidosis
- D - diarrhoea: gastrointestinal bicarbonate loss (e.g. high-output fistula)
- U - ureterostomies (urinary diversions): alters handling of cations/anions
- P - post hypocapnic state
- S - spironolactone (and hypoadrenalism / hypoaldosteronism)
Raised anion gap acidosis
Raised anion gap acidosis is due to accumulation of an unmeasured anion that consumes bicarbonate.
Often referred to as high anion gap metabolic acidosis (HAGMA).
A raised anion gap acidosis describes metabolic acidosis (pH < 7.35) with a raised anion gap (> 12 mEq/L).
In raised anion gap, there is consumption of bicarbonate due to accumulation of an unmeasured anion. There is no reciprocal increase in chloride concentration. It is usually due to renal disease, high lactate, ketones or several number of toxins. The causes of a raised anion gap acidosis can be remembered using the mnemonic MUDPILES

NOTE: lactate is produced during anaerobic respiration. It is a good marker of peripheral tissue perfusion.
Have comments about these notes? Leave us feedback