IIH
Notes
Overview
Idiopathic intracranial hypertension is a disorder characterised by features of raised intracranial pressure.
Idiopathic intracranial hypertension (IIH) is a disorder caused by chronically elevated intracranial pressure (ICP), which leads to the characteristic clinical features of headache, papilloedema (swollen optic discs) and visual loss. The actual cause of the condition remains unknown, but it primarily affects overweight women of childbearing age.
Several older terms have been used for IIH:
- Pseudotumor cerebri: cerebral tumours classically cause raised intracranial pressure
- Benign intracranial hypertension: renamed because the condition can be disabling and cause loss of sight
Epidemiology
The annual incidence of IIH is approximately 1-2 per 100,000 population.
The highest incidence of IIH is seen in women of childbearing age. In this group the incidence is as high as 21 per 100,000. The condition is strongly linked with obesity, and due to the rising obesity epidemic, rates are increasing. There is no major difference observed between ethnic groups.
Interestingly, although the incidence is much lower in men, they are at increased risk of visual loss.
Aetiology
The cause of IIH remains unknown.
IIH is idiopathic, meaning we do not know the underlying cause. However, weight and sex remain the most prominent risk factors for development of the condition.
Risk factors
- Weight: increased incidence in overweight and obese patients. Recent weight gain and higher body mass index is associated with higher risk of IIH
- Sex: much greater incidence in females
- Age: reproductive age
Associated conditions
IIH has been associated with several conditions and medications, although this only represents a small proportion of patients. In the literature there are many reported associations, but the evidence for many of these is limited.
The underlying association with some conditions may be related to a specific mechanism. For example, in hypercoagulable conditions there may be obstruction to venous outflow due to occult venous sinus thrombosis. Associations can be broadly divided into medication use, diet and systemic illnesses.
- Medication use: Growth hormone, tetracyclines, retinoids
- Dietary: excess vitamin A intake
- Systemic illnesses: sleep apnoea, hypercoagulable disorders, polycystic ovarian syndrome, systemic lupus erythematosus, Behçet syndrome, endocrinopathies (e.g. Addison’s, hypoparathyroidism).
Pathophysiology
The precise mechanism of raised intracranial pressure in IIH remains unknown.
The clinical manifestations of IIH occur due to raised ICP. The mechanisms leading to raised ICP is unknown, but several theories exist, which include:
- Intracranial venous hypertension: due to venous sinus narrowing/stenosis (may be a consequence of raised ICP rather than the direct cause). Thought to occur in distal transverse sinus segments
- Raised intra-abdominal pressure from central obesity: felt to increase central venous pressure and subsequently leads to an increase in ICP
- Altered sodium and water retention
- Impaired CSF reabsorption: occurring secondary to excess vitamin A or formation of micothrombi in the cerebral venous circulation
Clinical features
IIH is characterised by clinical features of raised intracranial pressure.
Any cause of raised ICP can lead to the characteristic features of headache (worse on lying down or bending over), papilloedema, and visual changes. Headache is the most common presenting feature in IIH.
IIH should be highly suspected in women of childbearing age who present with headache and papilloedema.
Symptoms
- Headache: worse on lying down or bending over. Often worse in the morning.
- Transient visual loss: usually last seconds, may be precipitated by position change. Unilateral or bilateral.
- Photopsia: refers to flashes of light.
- Tinnitus (pulsatile): refers to a ringing/buzzing noise in the ear
- Diplopia (double vision): typically on horizontal gaze. Most often due to unilateral or bilateral sixth cranial nerve (abducens) palsy. This is because of the long intracranial course of the sixth nerve, which is at risk of compression at the skull base with raised ICP.
- Visual loss (most concerning complication)
- Other features: neck, back and/or retrobulbar pain (i.e. pain behind the eyes).
Signs
- Papilloedema: refers to a swollen optic disc secondary to raised ICP. May be graded 0-5. Features include blurring of the disc margins, adjacent haemorrhage, swollen disc with oedema and obscuration of major vessels over the optic disc
- Visual loss: formal visual field testing is essential. Common patterns include enlarged blind spot, partial arcuate defect (small bow-shaped visual field defect, not crossing the midline), and peripheral field loss
- Sixth nerve palsy: causes a lateral rectus palsy with failed eye abduction on horizontal gaze
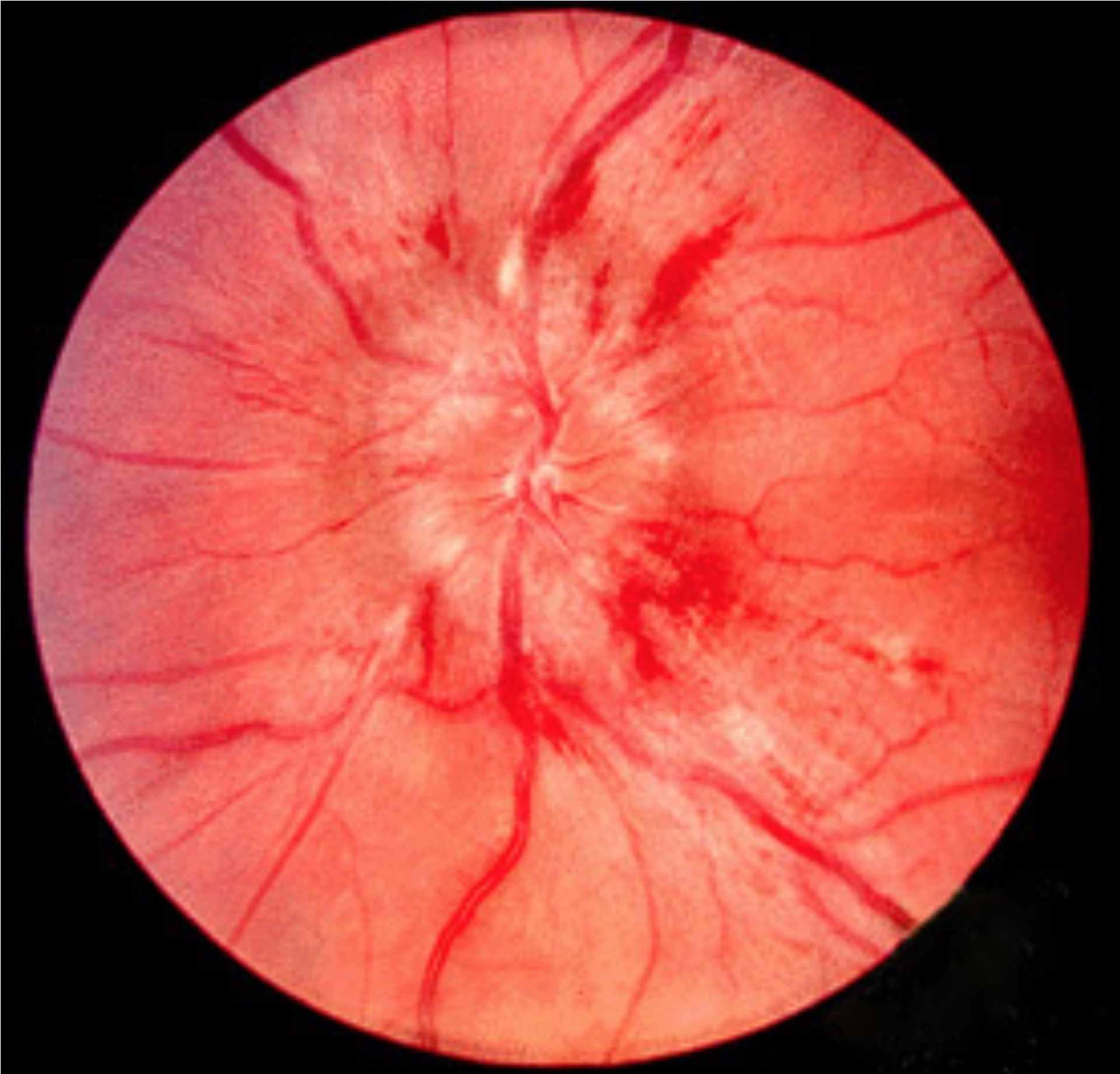
Retinal image showing papilloedema
Image courtesy of Jonathan Trobe, M.D (Wikimedia commons)
Diagnosis
Before making a diagnosis of IIH, it is important to exclude structural causes of raised ICP with neuroimaging.
The diagnosis of IIH is usually made by clinical features of raised ICP, identification of raised pressures on lumbar puncture and exclusion of an alternative cause using neuroimaging (e.g. space-occupying lesion, hydrocephalus, venous sinus thrombosis).
A formal diagnostic criteria is often used known as the modified Dandy criteria. This criteria has several components:
- Typical symptoms
- Absence of additional neurological features
- Raised ICP with normal cerebrospinal fluid composition
- Absence of another cause of intracranial hypertension
Differential diagnosis
Any condition causing raised ICP can lead to headache and papilloedema. Most of these conditions can be excluded using magnetic resonance imaging (MRI) including venography to exclude venous sinus thrombosis.
- Space-occupying lesion: primary CNS malignancy, metastatic deposit, cerebral abscess
- Venous outflow obstruction: venous sinus thrombosis
- Obstructive hydrocephalus: blockage to CSF leaving the ventricular system
- Decreased CSF reabsorption: subarachnoid haemorrhage, post-meningitis
- Increased CSF production: choroid plexus papilloma
Optic disc swelling
Optic disc swelling may be unilateral or bilateral, of which there are numerous causes.
The optic disc refers to the bright disc seen at the back of the eye on the nasal side of the retina. It is the location where all the ganglia cell axons exit and form the start of the optic nerve.
Optic disc swelling refers to the typical appearance of a swollen optic disc with raised borders, obscuration of major vessels running over the disc, and adjacent haemorrhages. These changes may be unilateral or bilateral.
There are numerous causes of optic disc swelling that may be divided into different categories:
- Intracranial conditions: cause optic disc swelling due to raised ICP. Known as papilloedema.
- Optic nerve pathologies (e.g. optic neuritis)
- Vascular conditions (e.g. retinal artery or vein occlusion)
- Conditions affecting the globe (e.g. uveitis)
Essentially, inflammation or ischaemia to the optic disc neurovascular supply can lead to damage and subsequent oedema seen as optic disc swelling. This may be due to direct involvement or secondary to increased pressure.
Investigations
Investigations are important to exclude an alternative cause for raised intracranial pressure.
Neuroimaging and lumbar puncture are the two critical investigations in the work-up of IIH. Most other causes of raised ICP can be excluded through neuroimaging.
Basic investigations
- Observations: BP is crucial in any patient presenting with headache
- Urinalysis: needed to exclude pregnancy and look for renal disease
- Bloods: basic laboratory tests (FBC, U&E, CRP, coagulation) are important to assess for clues of alternative diagnoses and to ensure it is safe to proceed with lumbar puncture.
- Ophthalmoscopy: basic bedside assessment to exclude papilloedema. Should be followed by formal ophthalmic assessment (including visual fields) if IIH is diagnosed or highly suspected.
Neuroimaging
Imaging of the brain with MRI with a venography phase (MRV) is needed to exclude alternative causes of raised ICP. CT imaging may be used acutely (e.g. for acute presentations to exclude serious alternative diagnoses such as intracerebral haemorrhage), or when MRI is not possible (e.g. incompatible pacemaker, claustrophobia).
Although neuroimaging is not used to make a diagnosis of IIH, there are several MRI features that can be suggestive of IIH.
Lumbar puncture
A lumbar puncture (LP) should be performed in all patients with suspected IIH if no contraindications. The diagnosis of IIH is based on measurement of the opening pressure (cmH20) taken in the lateral decubitus position (i.e. lying on your side). In IIH, the opening pressure is elevated. Basic CSF analysis should be completed in all samples including cell count, MC&S, protein and glucose. These are characteristically normal in IIH.
- Normal opening pressure (10-20 cmH20)
- Mildly elevated (20-25 cmH20): may be diagnostic of IIH if other characteristic features are present (e.g. MRI findings)
- Markedly elevated (>25 cmH20): consistent with IIH
Occasionally, the opening pressure may be falsely low due to other factors (e.g. Multiple attempts, hyperventilation, ICP-lowering medications). In addition, ICP pressure varies during the day. Therefore, if the opening pressure is low or mildly elevated and IIH is strongly suspected, a repeat LP should be considered.
Management
Weight loss and use of carbonic anhydrase inhibitors (e.g. acetazolamide) form the cornerstone of treatment.
Treatment of IIH is directed to alleviate symptoms and prevent irreversible visual loss.
Weight loss
Weight loss is the principle advice that is usually combined with medical therapy due to the time required to make significant improvements in weight. A low sodium weight loss programme should be advised. Severely obese patients may require weight reduction surgery to help achieve weight loss.
Serial lumbar punctures
Occasionally, serial lumbar punctures may be offered to patients. This involves performing an LP to remove excess CSF to reduce ICP. This should not be offered as a sole treatment and typically used as a temporary measure in patients who are likely to undergo surgery or cannot tolerate medical therapy.
Pharmacotherapy
The use of a carbonic anhydrase inhibitor (e.g. acetazolamide) is the treatment of choice for IIH.
- Acetazolamide 500 mg orally BD: titrated upward as needed
Carbonic anhydrase inhibitors are thought to work by reducing the amount of CSF production. This leads to a lower CSF pressure, less papilloedema, and improved visual testing. The BNF advises avoiding acetazolamide in pregnancy (particularly in the first trimester). These patients may require serial lumbar punctures if acetazolamide is felt too unsafe to use.
Other medications that may be used:
- Topiramate: anti-epileptic drug with activity against carbonic anhydrase
- Furosemide: loop diuretic that can be used as an adjunct to acetazolamide
Surgical treatment
Several surgical and newer interventional radiological procedures (e.g. venous sinus stenting) may be offered to patients with ongoing symptoms despite medical therapy. Some indications for surgery include worsening visual function despite medical therapy and intractable headache.
Main options include:
- Optic nerve sheath fenestration: small incisions are made to the optic nerve sheath to create a window that allows CSF to be released. This reduces pressure on the optic nerve head.
- Shunting: involves placement of a surgical shunt between CSF (e.g. ventricular system or lumbar spine) and another body cavity (e.g. peritoneum). Typical shunts include ventriculo-peritoneal or Lumbar-peritoneal. This helps to shunt CSF and reduce ICP.
Prognosis
The major long-term complication of IIH is permanent visual loss.
In the majority of patients, symptoms slowly worsen over time. Treatment can help improve or stabilise symptoms, but complete recovery is not possible in all patients. Recurrence (the development of symptoms after recovery or worsening after a period of stability) can occur in over a third of patients.
Longterm, the major concern is permanent visual loss. A subset of patients seem to have a more fulminant course with rapid progression to visual loss.
Last updated: July 2021
Have comments about these notes? Leave us feedback