Thyroid lumps
Notes
Overview
Approximately 90% of thyroid cancers present with a thyroid lump.
Though thyroid lumps most commonly represent benign growths in the form of cysts or toxic nodules in a small proportion of cases it is the presenting symptom of thyroid cancer.
This note focuses on the evaluation of unexplained thyroid lumps.
Referral
Patients presenting with unexplained thyroid lumps should receive urgent referral on a suspected cancer pathway.
Admit to hospital
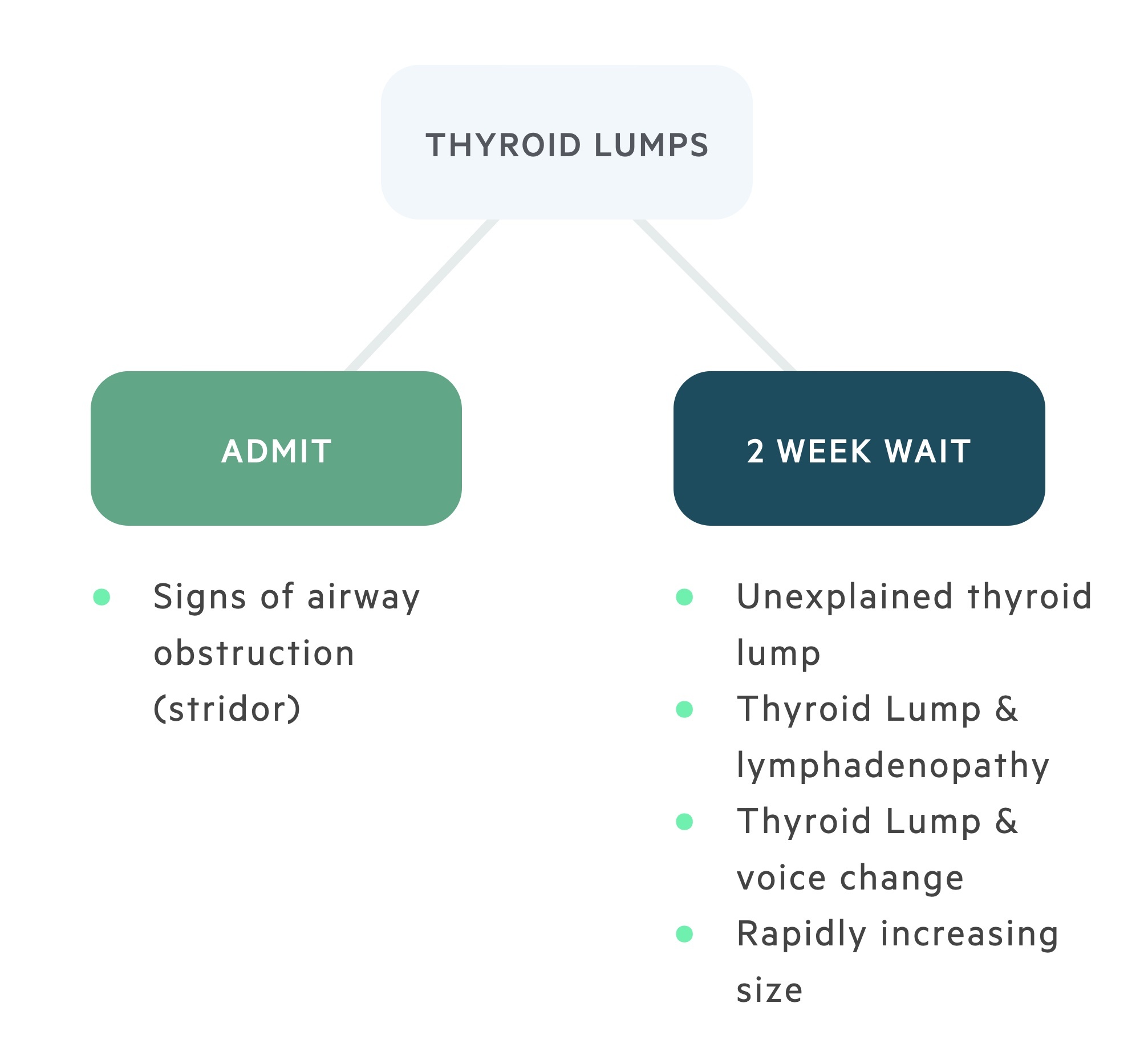
Patients with signs of tracheal compression such as stridor should be admitted to hospital for urgent review.
Two-week wait referral
- Any unexplained thyroid lump
- Thyroid lump associated with lymphadenopathy
- Thyroid lump with associated voice changes
- Rapidly increasing thyroid lump
Evaluation
Thyroid lumps should be investigated with clinical examination, ultrasound scan +/- fine needle aspiration cytology (FNAC).
1. Clinical Examination and thyroid function tests
All patients should have a full clinical review including a medical history (carefully evaluating family history and any exposure to carcinogens). This is followed by a clinical examination looking for signs of thyroid hormone imbalance and lymphadenopathy as well as evaluating the nodule itself.
2. Ultrasound scan
Ultrasound is the imaging modality of choice for thyroid lumps. A score U 1-5 is given based on the radiographical appearance of the nodule.
- U 1: Normal
- U 2: Benign
- U 3: Indeterminate/equivocal
- U 4: Suspicious
- U 5: Malignant
In addition, any lymphadenopathy, retrosternal extension or tracheal compression should be commented upon.
FNAC should be carried out on all U 3 – 5 lesions. Patients with U 1 and U 2 lesions do not need FNAC unless considered high risk for malignancy.
3. Fine needle aspiration cytology
FNAC allows for cytological assessment of a thyroid nodule. Reports may classify results as:
- Thy 1: Non-diagnostic
- Thy 2: Non-neoplastic
- Thy 3:
- Thy 3a: Atypical features
- Thy 3f: Follicular neoplasm suspected, cannot determine between follicular adenoma and follicular cancer
- Thy 4: Likely malignancy
- Thy 5: Malignancy
Inconclusive results
The results of the investigation of a thyroid lump are not always conclusive.
As a rule, if there is discordance between the clinical, radiographical or cytological results the case should be discussed at a specialist MDT.
Benign findings
Those with benign ultrasound appearances and Thy 2 cytology do not typically need follow up USS or FNAC unless the patient is considered high risk for malignancy.
Thy 1 (non-diagnostic cytology)
Those with indeterminate or suspicious USS and Thy 1 cytology should undergo repeat USS and FNAC and MDT discussion.
Discordant imaging and cytology
Those with indeterminate or suspicious USS and Thy 2 cytology should undergo repeat USS and FNAC and MDT discussion.
Thy 3a
Should be discussed at MDT. Normally further USS and FNAC is ordered. Further results should again be discussed at MDT.
Thy 3f and thy 4
Should be discussed at MDT. Typically, a diagnostic hemithyroidectomy is indicated to formally establish the diagnosis.
Have comments about these notes? Leave us feedback